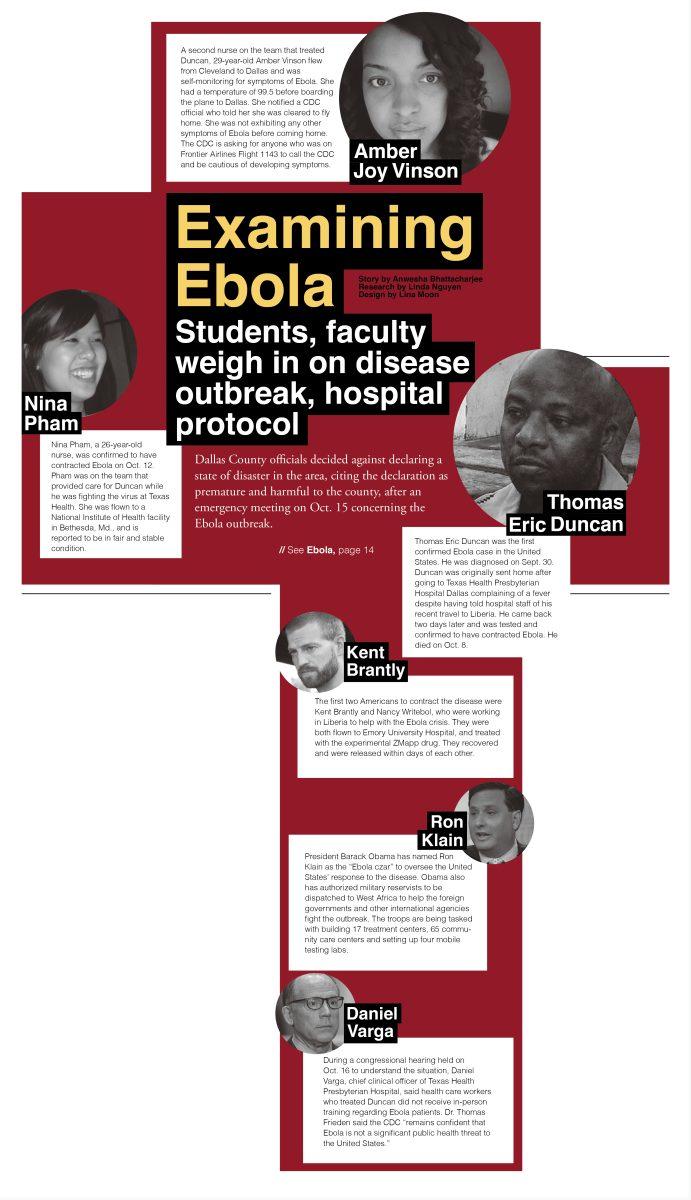
Students, faculty weigh in on disease outbreak, hospital protocol
Dallas County officials decided against declaring a state of disaster in the area, citing the declaration as premature and harmful to the county, after an emergency meeting on Oct. 15 concerning the Ebola outbreak.
The County has imposed travel restrictions on the 87 health workers who have been in contact with Thomas Eric Duncan, the first Ebola patient in the United States.
Duncan died on Oct. 8 at the Texas Health Presbyterian Dallas Hospital.
Those being monitored for exposure to Ebola will be asked to stay away from public transit for the 21 days they will be under observation, county officials said at the meeting.
“I think what they are doing now is that public health authorities are actively (surveying) these people,” said Paul Convery, health care management clinical professor. “(Centers for Disease Control and Prevention) initially asked them to call and check their temperature. Now, I think, (authorities) are sending a nurse out to everyone’s homes twice a day to actively check their temperature.”
The CDC should not have allowed Amber Vinson, the second nurse to be infected with the virus, to board the flight from Cleveland, Ohio, with a fever, Convery, a former first chief medical officer for Baylor Health Care Services, said.
Yet, if none of Duncan’s family members get infected by Ebola within the 21-day-quarantine that ends on Oct. 19, it implies that the disease can be contained provided health workers follow protocol while treating patients, Convery said.
“I don’t know what the gap was in the protocol about the protective gowns, but apparently they weren’t as 100 percent as they should have been,” he said.
The fact that the Ebola outbreak was successfully contained in Nigeria indicates that the spread of the virus can be stopped using contact tracing, said Olufunlola Arowolo, a public policy doctoral student from Nigeria.
Contact tracing starts with the first Ebola patient and traces and monitors anyone who was exposed to the patient, she said.
“They effectively contained and quarantined about 900 people, and no new cases of Ebola have been reported in about a month in Nigeria since the outbreak began. That’s the good news for Dallas because Dallas is implementing the same contact and trace method,” Arowolu said. “Not only that, Dallas also has more in terms of health care workers per capita citizens available, so I know that Dallas can definitely contain the issue.”
Student volunteers who work shifts at Texas Health each week are trained in following protocol in situations involving infectious diseases like Ebola, said a pre-med upperclassman who started volunteering at the hospital in August.
The source, who chose to remain anonymous out of concern of retaliation, said she had no contact with the Ebola patients in the hospital and volunteers like her are not allowed to work emergency room shifts anymore.
“I don’t feel concerned with in any way being in danger,” she said. “I think we all have had the proper training to know what the protocol is and we all work there, so I don’t feel that I am risk in any way.”
The hospital staff at Texas Health was not expecting a situation like this, which is why the response was probably slower, Convery said.
Even when protocols are in place, it takes some time for a smaller hospital to respond to what is expected to be a rare event, he said, so the CDC should have intervened earlier.
The problem lies in the fact that most small community hospitals across the nation don’t have the facilities and the physical space to keep a patient infected with Ebola in an isolated room that is surrounded by two empty rooms as is required, said John McCracken, clinical professor in health care management.
Research funding for the National Institute of Health has drastically decreased in the past few years, and the lack of an available Ebola vaccine or research on the virus might be, in some part, correlated to lack of NIH funding, Convery said.
“There was frankly not a lot of interest in Ebola in the United States a month ago,” he said. “Congress wasn’t doing a lot of talk about Ebola. I think some medical centers might have reacted differently to a first case that came in, but I would bet the vast majority of community hospitals would have reacted the way Presbyterian did.”
There is a possibility that a level-one trauma hospital such as Downtown Baylor or Parkland Hospital might have handled the case better, simply because they are used to seeing patients in extreme conditions in their emergency rooms, Convery said.
The roadmap ahead
After the initial scare, hospitals across the nation are gearing up to prepare for a possible outbreak ensuring there is sufficient protective gear and adequate training for the hospital staff, Convery said.
“I was up in Springfield, Ill., a town of 100,000 (people), and they’re having discussions and drills and beginning to understand how to prepare for it,” he said.
Since the first Ebola case developed in Dallas, even pharmacy technicians at the Baylor Hospital in McKinney have started wearing masks, aprons and gloves, said Raisha Shaeef, a pre-med and biochemistry senior who works there.
Texas Health is receiving a lot of negative press, and situations are tense at the hospital right now, the anonymous volunteer at the hospital said.
The nurse morale is low, and the hospital staff is under the public glare, a situation that is not likely to change any time soon, Convery said.
“I begrudge the news, the talking heads, because they always make any event, no matter what it is, sound like it’s the precursor to the end of the world,” McCracken said.
The average person in Dallas is not constantly looking over his or her shoulder for Ebola, and there is little panic among the people, unlike what the media would like to project, he said.
The media’s reaction is not unexpected, the anonymous pre-med student said. People who work in a hospital environment can understand the reality of the ground-level risks involved, but it can be difficult for the general public that is relatively unaware of the disease characteristics and risks to stay calm at a time like this.
“The problem with Ebola is that it’s a virus, therefore, non-treatable by antibiotics,” McCracken said. “Second, the fatality rate is very high, about 80 to 85 percent. The transmission mechanism isn’t well understood. (Researchers) don’t think that it is transmuting to be transmitted through the air, but they don’t know.”
However, a handful of people of the 305 million living in the United States have been infected with Ebola, which is a very insignificant number statistically, he said.
“I will say this though: There are fewer than 10,000 reported cases of Ebola (in the world), although, probably (cases in) West African countries are underreported,” McCracken said. “You still have much higher risk of fatality from flu than you do from Ebola. It’s much more important to get a flu shot than it is trying to prevent yourself from Ebola.”
Once the disease is contained, the federal government will conduct several investigations into what went wrong at Texas Health, he said.
The incident has provided students with several angles for future study, McCracken said.
The breakdown of systems and procedures and the breach of protocol at Texas Health is one obvious perspective for analysis, he said. The other is the study of Texas Health’s public response, which will be significant not only for the hospital, but also for other providers, McCracken said.
“The biggest lesson that we learned is how to present a disaster like this to the public and how to put a public face on it, and what to say, when to say it and how to say it,” he said.
In the meantime, countries in Europe have to figure out how to prevent the large-scale migration from Guinea, Sierra Leone, Liberia and Ivory Coast to Belgium, Spain and other European Union countries as people from West Africa attempt to flee the epidemic or travel for treatment, McCracken said.
The migration barriers, however, do not provide any premise for discrimination on the basis of nationality in the United States, Convery said. This epidemic is truly a global problem, and every country needs to step up its response to contain it, he said.
The United States will soon send several hundred troops to Liberia to help build infrastructure that will be used to contain the Ebola outbreak, and the country will have to plan a contingency for when the soldiers return and situations where they might be infected, Convery said.
At the moment, close to 200 people are being monitored across the country for possible Ebola infections, and there has been no further escalation in Dallas, he said.
“This is one of those times when you want to wait and see,” McCracken said.